
A regular series on the latest clinical studies from around the world – and what they mean ‘in practice’ – compiled and written by Clare GP Dr Ray O’Connor
Vaccines
Why are vaccines not giving long-term protection against Covid-19? Most studies of immunity to SARS-CoV-2 focus on the circulating antibody, giving limited insights into mucosal defences that prevent viral replication and onward transmission. This follow-up study1 looked at nasal and plasma antibody responses one year after hospitalisation for Covid-19, including a period when SARS-CoV-2 vaccination was introduced. Plasma and nasosorption samples were prospectively collected from 446 adults hospitalised for Covid-19 between February 2020 and March 2021.
IgA and IgG responses to SARS-CoV-2, Delta and Omicron (BA.1) variants were measured and compared with plasma neutralisation data. There was a decline in nasal IgA responses nine months after infection and minimal impact of subsequent vaccination. This may explain the lack of long-lasting nasal defence against reinfection and the limited effects of vaccination on transmission.
Dr Ray O’Connor
The authors conclude that future vaccines will need to substantially boost nasal IgA if they are to fully prevent infection and transmission. To date, intranasal and aerosolized vaccines have shown the most promise in doing so. The authors also conclude that it is essential to prioritise development of mucosal vaccines which can provide better protection against respiratory infections including SARS-CoV-2.
A literature review2 studied the durability of the antibody response after SARS-CoV-2 infection and the role of antibodies in protection against reinfection. Data Sources were MEDLINE (Ovid), EMBASE, CINAHL, World Health Organization Research Database, and reference lists from December 16, 2021 through July 8, 2022, with surveillance through August 22, 2022.
 The conclusions were that evidence for a sustained antibody response to SARS-CoV-2 infection is considerable for both Delta and Omicron variants. Prior infection protected against reinfection with both variants, but, for Omicron, protection was weaker and waned rapidly. However, this information may have limited clinical applicability as new variants emerge.
The conclusions were that evidence for a sustained antibody response to SARS-CoV-2 infection is considerable for both Delta and Omicron variants. Prior infection protected against reinfection with both variants, but, for Omicron, protection was weaker and waned rapidly. However, this information may have limited clinical applicability as new variants emerge.
Drug treatment
For those people who contract Covid-19 in the community, should we consider treatment with antiviral agents? The safety, effectiveness, and cost-effectiveness of molnupiravir, an oral antiviral medication for SARS-CoV-2, has not been established in vaccinated patients in the community at increased risk of morbidity and mortality from Covid-19.
The PANORAMIC group studied whether the addition of molnupiravir to usual care reduced hospital admissions and deaths associated with Covid-19 in this population.3 PANORAMIC was a UK-based, national, multicentre, open-label, multigroup, prospective, platform adaptive randomised controlled trial. Eligible participants were aged 50 years or older—or aged 18 years or older with relevant comorbidities—and had been unwell with confirmed Covid-19 for five days or fewer in the community.
Participants were randomly assigned (1:1) to receive 800mg molnupiravir twice daily for five days plus usual care or usual care only. Between December 8, 2021, and April 27, 2022, 26,411 participants were randomly assigned, 12,821 to molnupiravir plus usual care, 12,962 to usual care alone.
The conclusion was that Molnupiravir did not reduce the frequency of Covid-19-associated hospitalisations or death among high-risk vaccinated adults in the community.
References:
- Liew F et al. SARS-CoV-2-specific nasal IgA wanes 9 months after hospitalisation with COVID-19 and is not induced by subsequent vaccination. eBioMedicine 2022;104402. Published online: https://doi.org/10.1016/j.ebiom.2022.104402. (In press: Published online January 2023).
- Kolmer HK et al. Major Update 2: Antibody Response and Risk for Reinfection After SARS-CoV-2 Infection—Final Update of a Living, Rapid Review. Ann Intern Med. doi:10.7326/M22-1745.
- Butler C et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): an open-label, platform adaptive randomised controlled trial. Published online December 22, 2022. https://doi.org/10.1016/S0140-6736(22)02597-1. Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
**********
Standards of Care in Diabetes
An updated version of the document Standards of Care in Diabetes has just been published by the American Diabetes Association.1 The target audience for the Standards of Care document includes primary care physicians, endocrinologists, nurse practitioners, pharmacists, dietitians, diabetes care and education specialists. The Standards of Care document also provides guidance to specialists caring for people with diabetes and its multitude of complications, such as cardiologists, nephrologists, emergency physicians, internists, paediatricians and psychologists.
 The recommendations are informed by a systematic review of evidence and an assessment of the benefits and risks of alternative care options. The Standards of Care subcommittee for each section creates an initial list of relevant clinical questions that is reviewed and discussed by the expert panel.
The recommendations are informed by a systematic review of evidence and an assessment of the benefits and risks of alternative care options. The Standards of Care subcommittee for each section creates an initial list of relevant clinical questions that is reviewed and discussed by the expert panel.
In consultation with a systematic review expert, each subcommittee devises and executes systematic literature searches. For the 2023 Standards of Care, PubMed, Medline, and EMBASE were searched for the time periods of June 1,2021 to July 26, 2022.
The first section summarises revisions since the last document. These are extensive and take into account improvements in technology, changes in medication and understanding of the disease.
Many treatment goals are updated. For example, people with diabetes and hypertension qualify for antihypertensive drug therapy when the blood pressure is persistently elevated above 130/80mmHg. The on-treatment target blood pressure goal is <130/80mmHg, if it can be safely attained.
The whole document is 298 pages long and serves as a useful reference.
Type 2 diabetes in young people
Not all that long ago, type 2 diabetes was known as ‘Maturity Onset Diabetes Mellitus’ because it was thought to occur mainly in older people. In more recent times unfortunately, it has been occurring in younger people due mainly to lifestyle factors such as obesity, poor diet and low levels of physical activity. This study2 sought to estimate the global burden of type 2 diabetes in adolescents and young adults (aged 15-39 years) from 1990 to 2019 in 204 countries and territories. It was a systematic analysis of the Global Burden of Disease Study 2019.
The main outcomes measures were age standardised incidence rate, age standardised disability adjusted life years (DALY) rate, and age standardised mortality rate for type 2 diabetes and proportional DALY attributable to different risk factors.
 The results were that over the study period, there were significant increases in age standardised incidence rate and age standardised DALY rate were found for type 2 diabetes in adolescents and young adults globally.
The results were that over the study period, there were significant increases in age standardised incidence rate and age standardised DALY rate were found for type 2 diabetes in adolescents and young adults globally.
Age standardised incidence rate (per 100 000 population) increased from 117.22 in 1990 to 183.36 in 2019, and age standardised DALY rate (per 100 000 population) increased from 106.34 in 1990 to 149.61 in 2019. The age standardised mortality rate (per 100 000 population) was modestly increased from 0.74 in 1990 to 0.77 in 2019.
When grouped by countries with different socio-demographic indexes, countries with a low-middle and middle socio-demographic index had the highest age standardised incidence rate and age standardised DALY rate in 2019, whereas countries with a low socio-demographic index had the lowest age standardised incidence rate but the highest age standardised mortality rate. Women generally had higher mortality and DALY rates than men at ages <30 years, but differences between the sexes were reversed in those aged >30 years except in countries with a low socio-demographic index (i.e. poor countries).
The study concluded that early onset type 2 diabetes is a growing global health problem in adolescents and young adults, especially in countries with a low-middle and middle socio-demographic index. A greater disease burden in women aged <30 years was found.
Specific measures are needed in countries with different levels of socioeconomic development because of the variable attributable risk factors for type 2 diabetes in adolescents and young adults.
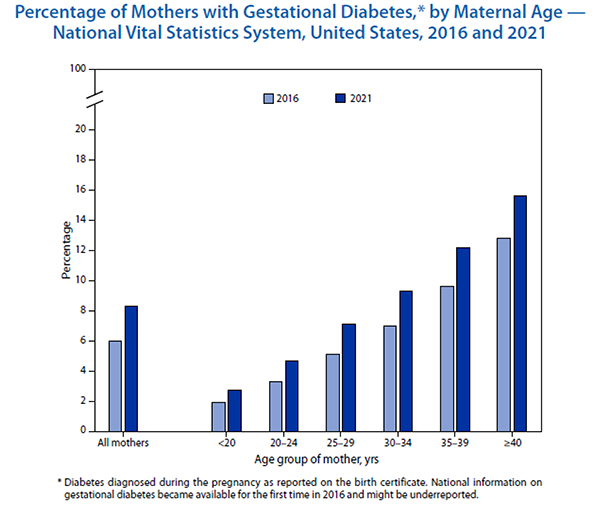
Gestational Diabetes Mellitus
Gestational Diabetes Mellitus (diabetes in pregnancy) is being seen increasingly in practice. How common is it and is it affected by age? These questions were clearly answered by a paper published in the Morbidity and Mortality Weekly Report from the Centers for Disease Control in USA.3 The authors found that the percentage of mothers giving birth who received a diagnosis of gestational diabetes increased from 6.0 per cent in 2016 to 8.3 per cent in 2021. Increases in gestational diabetes were seen in each maternal age group, and rates rose steadily with maternal age; in 2021, the rate for mothers aged ≥40 years (15.6 per cent) was nearly six times as high as the rate for mothers aged <20 years (2.7 per cent). The data are summarised very nicely in the graph above.
References:
- ElSayed NA, Aleppo G, Aroda VR, et al., American Diabetes Association. Introduction and methodology: Standards of Care in Diabetes—2023. Diabetes Care 2023;46(Suppl. 1):S1–S4.
- Xie J et al. Global burden of type 2 diabetes in adolescents and young adults, 1990-2019: systematic analysis of the Global Burden of Disease Study 2019. BMJ 2022;379:e072385 http://dx.doi.org/10.1136/bmj‑2022‑072385.
- Martin JA et al. Percentage of Mothers with Gestational Diabetes, by Maternal Age — National Vital Statistics System, United States, 2016 and 2021. MMWR / January 6, 2023 / Vol. 72 / No. 1. P16.
**********
Ambulatory blood-pressure monitoring (ABPM)
Ambulatory blood-pressure monitoring (ABPM) has become less frequent in primary care since the Covid-19 pandemic, with home blood- pressure monitoring (HBPM) often the preferred alternative; however, HBPM cannot measure night-time blood pressure (BP), and patients whose night-time BP does not dip, or rises (reverse dipping), have poorer cardiovascular outcomes.
 This study1 looked at the importance of measuring night-time BP when assessing individuals for hypertension. It was a retrospective cohort study of two patient populations — namely, hospital patients admitted to four UK acute hospitals located in Oxfordshire, and participants of the BP in different ethnic groups who were recruited from 28 UK general practices in the West Midlands.
This study1 looked at the importance of measuring night-time BP when assessing individuals for hypertension. It was a retrospective cohort study of two patient populations — namely, hospital patients admitted to four UK acute hospitals located in Oxfordshire, and participants of the BP in different ethnic groups who were recruited from 28 UK general practices in the West Midlands.
Among the hospital cohort, 48.9 per cent patients were ‘reverse dippers’, with an average day–night systolic BP difference of +8.0mmHg. Among the community cohort, 10.8 per cent of patients were reverse dippers, with an average day–night systolic BP difference of +8.5mmHg.
Non-dipper and reverse-dipper phenotypes both had lower daytime systolic BP and higher night-time systolic BP than the dipper phenotype. The authors concluded that not measuring night-time BP puts reverse dippers (those with a BP rise at night-time) at risk of failure to diagnose hypertension. As a result of this study, it is recommended that GPs should offer ABPM to all patients aged ≥60 years as a minimum when assessing for hypertension.
Hypertension with CV Disease
What about those with hypertension and established cardiovascular disease (CVD)? These people are known to be at particularly high risk, so reducing blood pressure to below standard targets may be beneficial. This strategy could reduce cardiovascular mortality and morbidity but could also increase adverse events.
The optimal blood pressure target in people with hypertension and established cardiovascular disease remains unknown. This Cochrane review looked at whether lower blood pressure targets (systolic/diastolic 135/85mmHg or less) are associated with reduction in mortality and morbidity compared with standard blood pressure targets (140mmHg to 160mmHg/90mmHg to 100mmHg or less) in the treatment of people with hypertension and a history of cardiovascular disease (myocardial infarction, angina, stroke, peripheral vascular occlusive disease).
They found there is probably little to no difference in total mortality and cardiovascular mortality between people with hypertension and cardiovascular disease treated to a lower compared to a standard blood pressure target. There may also be little to no difference in serious adverse events or total cardiovascular events.
This suggests that no net health benefit is derived from a lower systolic blood pressure target. They found very limited evidence on withdrawals due to adverse effects, which led to high uncertainty.
At present, evidence is insufficient to justify lower blood pressure targets (135/85mmHg or less) in people with hypertension and established cardiovascular disease.2 Several trials are still ongoing, which may provide an important input to this topic in the near future. ![]()
References:
- Armitage LC et al. Diagnosing hypertension in primary care: a retrospective cohort study to investigate the importance of night-time blood pressure assessment. Br J Gen Pract 2022; https://doi.org/10.3399/BJGP.2022.0160.
- Saiz LC, Gorricho J, Garjon J, et al. Blood pressure targets for the treatment of people with hypertension and cardiovascular disease. Cochrane Database Syst Rev. 2022 Nov 18;11(11):CD010315. doi: 10.1002/14651858.CD010315.pub5. (Systematic review).
Discover more from PressNewsAgency
Subscribe to get the latest posts sent to your email.