Get the latest on coronavirus. Sign up to the Daily Brief for news, explainers, how-tos, opinion and more.Â
The nation has been given a glimmer of hope in the fight against coronavirus with the news that up to 30 million doses of a Covid-19 vaccine will be made available to the UK by September – if human trials by Oxford University prove successful.
Business secretary Alok Sharma said earlier this week that Oxford was one of the world’s forerunners in the race for a vaccine and that clinical trials were “progressing well†with all phase one participants having received their vaccine doses on schedule.
But what exactly is the coronavirus vaccine trial, what are scientists trying to find out and what do participants have to do as part of their involvement in their involvement in the clinical study?Â
What is the purpose of the human trial of the coronavirus vaccine?
The aim is to test a new vaccine against Covid-19 in healthy volunteers.
The study will assess whether healthy people can be protected from coronavirus with this new vaccine called ChAdOx1 nCoV-19.
It will also provide valuable information on safety aspects of the vaccine and its ability to generate good immune responses against the virus.
Who can take part in the human trial of the vaccine?
Up to 1,102 participants have been recruited across multiple sites in Oxford, Southampton, London and Bristol.
Volunteers must be aged between 18 and 55 and cannot have tested positive for Covid-19. They must be in good health and be based in one of the recruiting areas.
They must not be pregnant, intending to become pregnant, or breastfeeding during the study.
Participants cannot have previously taken part in a trial with an adenoviral (relating to this particular group of viruses) vaccine or received any other coronavirus vaccines.
Jack Sommers
Jack Sommers, 34, who is taking part in the Covid-19 vaccine trial.
Jack Sommers, 34, who lives in south-west London, volunteered for the trial the day after discovering he was being made redundant from his job.
He told HuffPost UK he realised he was the perfect candidate for the study and wanted to do something useful.
“I am healthy, have had an uneventful medical history and have had no symptoms of coronavirus,†he said. “And as I live alone, there is no risk of me infecting vulnerable people or frontline workers.
“I also only live a 10-minute walk away from St George’s Hospital in Tooting which is one of the sites for the trial so I knew taking part would be relatively easy.
“For me to take part seemed a no-brainer and I knew how important it was.â€Â
Why are human volunteers needed for the trial?
Until now, this Covid-19 vaccine has only been tested on laboratory mice and other animal species and this trial is the first time it has been given to humans.
The vaccine was developed in less than three months by a team at Oxford University and, although there has been pre-clinical research, it needs to be tested on humans and data needs to be evaluated.
Scientists need to demonstrate the vaccine actually works and stops people getting infected with coronavirus before it can be rolled out to the wider population.
When my grandkids ask: ‘What did you do during the Great Coronavirus Lockdown Grandad?’ I’ll be able to say: ‘I did this.’ It makes me feel I am doing something worthwhile. Jack Sommers
“Without people willing to take part, new vaccines wouldn’t be developed,†said Jack.
“I know there are some theoretical risks, but I have the greatest faith in the doctors and scientists and feel safe in their hands.â€
Jack added: “In years to come when we all look back and talk about this time and my grandkids ask: ‘What did you do during the great coronavirus lockdown grandad?’ I’ll be able to say: ‘I did this.’ It makes me feel I am doing something worthwhile.â€
How does the trial work and what do participants have to do?
Half the volunteers taking part in the trial will be injected with the prospective coronavirus vaccine while the other half will be given a meningitis vaccine that will be used as a control for comparison.
Volunteers will not know which vaccine they have received.
Jack said: “I completely understand there needs to be a placebo in clinical trials and, for this study, they wanted something stronger which is why they have used the meningitis vaccine.
“As far as I am concerned, I’m quids in. Whichever jab I have received, I’ve either been vaccinated against coronavirus or meningitis.â€
After filling in paperwork, giving blood and urine samples for testing and watching a safety video, Jack was accepted on the trial.
He returned to hospital to receive an injection in his shoulder, which he described as “exactly like getting your holiday jabsâ€.Â
Jack Sommers
Jack Sommers, 34, who is taking part in the Covid-19 vaccine trial.
Jack and the other participants were sent home with a thermometer and a measuring tape to measure any potential swelling of the injection site.
Participants were also asked to fill in an e-diary to record any symptoms they experience in the first seven days after receiving the vaccine and to report if they feel unwell over the following three weeks.
Jack reported experiencing a very mild throat tickle the day after the injection and, the next day, he had a slightly raised temperature.
He is now in the second week following the vaccination and simply logs on to the e-diary every day and answers two straightforward questions on whether he has symptoms.
“I only have to give any details if I feel anything different, but I haven’t as yet,†he said.
Jack will return back to the trial site one month on from to have tests.
There will then be another visit and check-up six months on from the injection and an optional one a year on from the vaccination.
Jack said: “The symptoms for me have been very mild so I have barely suffered any inconvenience to my life at all.
“I had to input my temperature into the online diary for the first week, but now all I have to do is spend about five seconds putting: ‘No, I don’t have any symptoms.’â€
At the start of the trial, a separate small group of 10 volunteers were also recruited to receive two doses of the Covid-19 vaccine four weeks apart.
This is to assess different reactions to a second dosage and establish both safety and how the immune response differs from those receiving a single dose.
Meyer & Meyer via Getty Images
A file image of a doctor filling a syringe with a vaccine.
What is the vaccine being tested?
The vaccine being tested in this research study is called ChAdOx1 nCoV-19.Â
It is made from a virus (ChAdOx1), which is a weakened version of a common cold virus (adenovirus) that causes infections in chimpanzees. It has been genetically changed so that it is impossible for it to grow in humans.
Scientists are hoping to make the body recognise and develop an immune response to the spike protein on the outside of the virus to stop it entering human cells and so prevent infection.
The main focus of the study is to find out if this vaccine is going to work against Covid-19, ensure it won’t cause unacceptable side effects, and see if it induces good immune responses.Â
What happens next?
There are a lot of complex stages in vaccine development according to Sarah Gilbert, professor of vaccinology at Oxford University’s Jenner Institute.
She says they will increasingly immunise more people to check for safety and immune response to the vaccine in older people as well as younger ones.
“This is particularly important because it’s the older population that we really need to protect with a vaccine,†she said. “But with vaccines in general you often get a lower immune response as the immune system ages. So, we need to find out how well this vaccine works in older people compared to younger people by measuring the immune response to the vaccination.â€Â
University of Oxford
Sarah Gilbert, professor of vaccinology at the Jenner Institute at Oxford University.
She said the research team would also be checking if the vaccine actually protects people against Sars-CoV-2, the virus that causes Covid-19.
“People don’t know which vaccine they’re having and, over time, as people become infected or have symptoms of coronavirus, they’ll come to us to get tested.
“When enough people have become positive for the coronavirus, the statisticians will look at which groups those people are in, to find out whether they are in the group that had the coronavirus vaccine, or whether all positive cases are in the group that had the meningitis vaccine.
“We’re hoping for the infections to happen only in the meningitis vaccine group. And if that’s the case we will then be able to say that this vaccine works, at least in the age range we have vaccinated, and we can then start expanding the studies and we can start to apply for emergency use licensure so that the vaccine can be used more widely.â€Â
Will people in the UK get access to the vaccine first if it is successful?
The UK will be first in line for 30m doses of Oxford University’s coronavirus vaccine by September if it passes trials, business secretary Alok Sharma has said.
He announced a deal had been struck between Oxford University and pharmaceutical giant AstraZeneca meaning that 30m doses would be made available by September for the UK as part of an agreement to deliver 100m doses in total, if ongoing trials succeed.
“The UK will be first to get access,†said Sharma. “Once a breakthrough is made, we need to be ready to manufacture a vaccine by the millions.â€
He also announced a further £84m in funding to accelerate the work currently being done in vaccine trials at Oxford University and at Imperial College.
Is there a chance the vaccine won’t work?
Despite putting considerable investment into vaccine development, the government has cautioned that an effective coronavirus vaccine may never be found.
Gilbert agrees that, while she believes the prospects of developing a workable vaccine are good, nothing is certain.
“Nobody can be absolutely sure it’s possible to produce a successful vaccine, that’s why we have to do trials to find out.
“I think the prospects are very good but, clearly, it’s not completely certain.â€
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
NEW DELHI — On May 17, the day the Union government significantly relaxed India’s punitive national lockdown, the country recorded the largest single day spike in fresh cases of and fatalities due to the novel coronavirus.
The same day, Union Health Minister Harsh Vardhan said India had hit the 80,000 cases mark in 106 days after recording its first infection while many developed nations took just 44-66 days to reach that mark. The health ministry said the number of COVID-19 cases in the country were now doubling every 13.6 days, an improvement over the past fortnight, when cases were doubling every 11.5 days.
These cautiously upbeat statements and the easing of lockdown restrictions juxtaposed against the grim news of steadily spiking infections and fatalities reveal a worrying pattern: The Union government is using incomplete national-level data to justify arbitrary policy decisions, defend its record, and underplay the extent of the COVID-19 crisis.
HuffPost India’s analysis of publicly available data, local health bulletins, government documents, interviews with district and state-level officials, and infectious disease experts suggests that these imperfect numbers at best, offer an underestimate of the coronavirus’s spread, and at worse, form the basis for misleading conclusions to support arbitrary policy decisions.Â
Despite widely acknowledged inconsistencies and limitations of these data —the numbers are significantly dependent on India’s testing strategies and availability of testing infrastructure— senior health officials continue to display graphs at press conferences to give the illusion that the government is aware of how the pandemic is unfolding in real-time. Future projections of COVID-19 cases shared with states by the NITI Ayog and the Union Health Ministry are sometimes wildly divergent.
On April 11 for instance, the health ministry justified Prime Minister Narendra Modi’s controversial decision to lockdown the entire country without prior warning or planning, by presenting a graph that claimed India would have witnessed 800,000 cases by April 15 had the lockdown not been imposed. Experts questioned this projection, noting there was no explanation to justify these numbers. Â
Source: Health Ministry Press Conference, April 11
On April 11, the health ministry claimed, with little evidence, that India would have witnessed 820,000 cases of COVID-19 had the lockdown not been imposed. Experts have questioned this estimate.
If the decision to impose the national lockdown on March 24 was justified on the basis of such ambiguous data and modeling, the government has offered no empirical explanation for the subsequent extension or easing for the lockdown.
To be sure, countries across the world have struggled to collate robust coronavirus statistics. But India, with its poor track record of data governance, has its own peculiar issues: Statistics routinely shared with the public by both the union government and state governments are compromised by long delays in processing tests, questionable interpretation of available numbers, and rudimentary modelling of India’s coronavirus crisis. This makes it hard to understand how the disease will spread over the next several days, weeks and months, when and where the number of cases will peak, and if India’s patchwork system of public and private healthcare will hold up.
The crisis in India’s data gathering, and the way this data is deployed by policymakers, is likely to become more pronounced in the coming weeks as travel restrictions ease and COVID-19 cases spike.
India’s narrow testing strategies and the limited testing infrastructure mean that even the highest levels of government do not have a real-time picture of how the pandemic is unfolding across the country.
The largely rosy view from the Union Health Ministry in New Delhi obscures vivid regional disparities across every metric used to measure the progress of the virus; making the case that states should have been given more freedom to devise their COVID-19 responses — including when and where to impose strict lockdowns — from the very beginning.
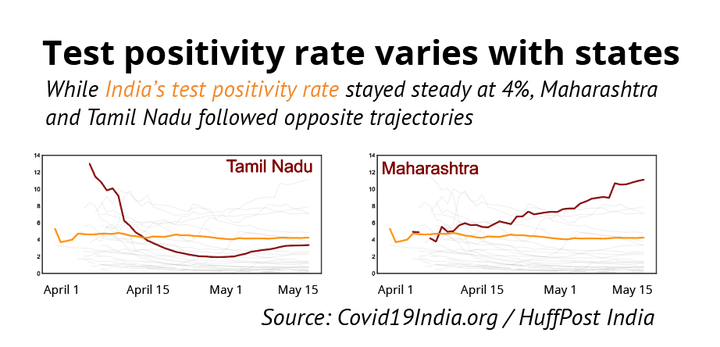
For instance, HuffPost India’s analysis suggests the country’s steady test positivity rate of 4% for several weeks (meaning there 4 positive cases out of every hundred tests conducted in India) appears to be a case of divergent regional trends cancelling each other out: On 10th April, Tamil Nadu’s test positivity rate was 10.8%, while Maharashtra’s was only 3.8%. By 16 May, Maharashtra’s positivity rate rose rapidly to 11%, while Tamil Nadu moved in the opposite direction to 3.4%. All this while, the national figures stayed flat at 4%.Â
HuffPost India
While Union Health Ministry officials in Delhi continue to use aggregated national-level data to insist that the spread of the virus has been contained, granular data shows wide divergence among states.
Yet, the Union Health Ministry continues to speak in large, aggregate numbers that are essentially meaningless and devoid of context, and are occasionally used to present ludicrous scenarios.Â
“It makes a mockery of our response to the pandemic,†said Gautam Menon, a professor of physics and biology at Ashoka University, who researches infectious disease modelling. “What India and the world needs now is transparency and clarity regarding what is going on.â€
“I recognise the desire of the government to present a positive face, but this should not be done by concealing data, by not revealing details of its preparation, by refusing to respond to genuine questions about its data and so on,†Menon said. Rather, Menon said, the government should maintain the trust of the public by being transparent in its presentation of facts.
Delayed tests
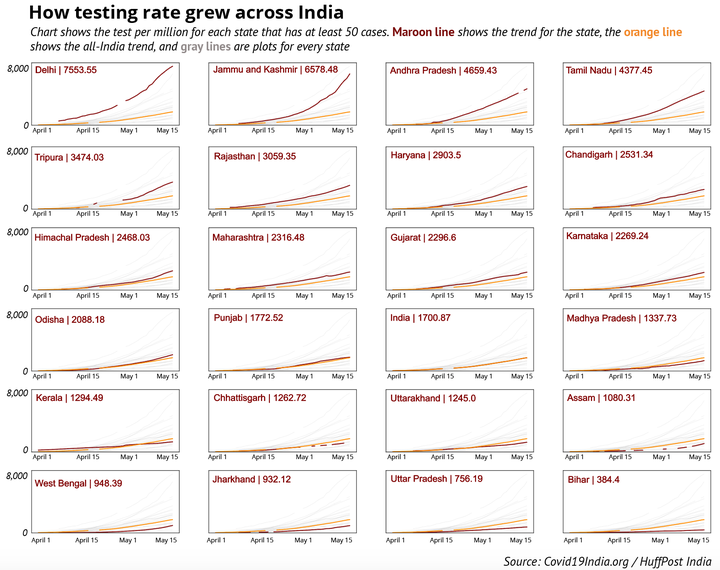
India’s testing trajectory is two-pronged. One one hand, the country has consistently ramped up testing, and now has a daily capacity to test over one lakh samples a day—only six countries have conducted more than India’s 2.4 million tests.Â
On the other hand, India’s vast population has meant the testing rate of 1,744 per million remains low. Of 149 countries to have reported at least 100 cases, only 33 have a lower testing rate than India, according to Worldometer.Â
HuffPost India
testing rate
As long as the testing remains limited, the number of confirmed COVID-19 cases will have limited meaning as well: increased testing might reveal more positive cases, but will not help us map the spread of the virus.
To understand how India’s attempts to contain the coronavirus have been hampered by the country’s persistent inability to test enough people and deliver timely results, consider Madhya Pradesh’s Ashok Nagar district, home to about a million people.
Ashok Nagar is a “green†district with only 2 COVID-19 cases thus far, but with train services resuming, the region expects thousands of workers stranded across the country to return home soon.
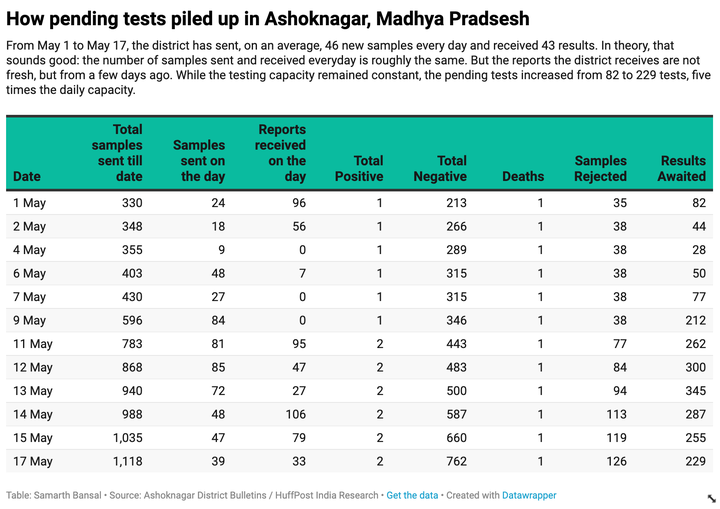
In the first day of May, Ashok Nagar had collected a total of 330 samples and received reports of 248 patients; the results of 82 samples were pending from April. By the 13th of May, the district had sent 940 samples, but a bottleneck in analysing these samples meant the number of pending samples had ballooned to 345 — more than four times the number of pending samples from a fortnight ago.Â
In a phone call, Ashok Nagar’s Chief Health and Medical Officer JR Trivediya confirmed the delays in receiving test results. Ashok Nagar’s experience can be extrapolated across Madhya Pradesh, say health activists.
HuffPost India
A daily breakdown of testing data in Ashoknagar, Madhya Pradesh, shows how quickly a backlog of test results can pile up.
“The backlog of pending samples awaiting results has been increasing at a rapid pace,†said Bhopal-based activist Amulya Nidhi of Jan Swasthya Abhiyan in a letter sent to the Union health secretary on May 6. “Patients were waiting for their test results and there are multiple instances of deaths happening before test results arrived.â€
As of April 25, for instance, Madhya Pradesh had 9,021 pending samples against a daily testing capacity of around a thousand tests. This meant test results — on average — were delayed by nine days. The following day, Madhya Pradesh simply stopped publishing data on the number of pending tests.
In a fast-moving pandemic like COVID-19, this delay has significant real-world effects: For a health official in Madhya Pradesh hoping to use the data to figure hotspots, trace contacts, and prepare for an influx of patients, the state’s infection rate data would be obsolete well before it reached his desk.Â
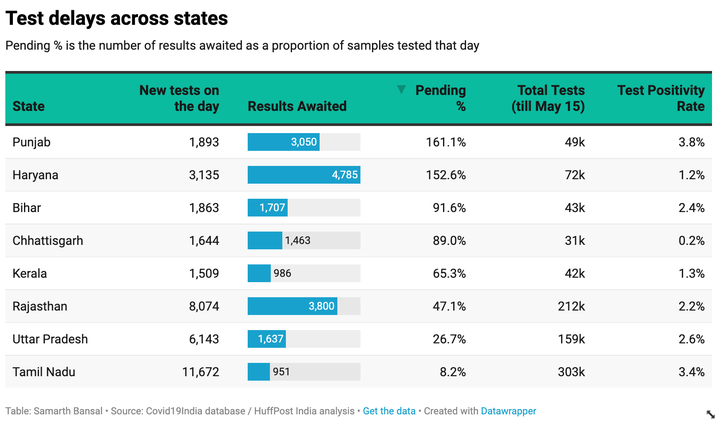
Madhya Pradesh is not alone in hiding uncomfortable statistics. HuffPost India found only eight of the twenty large states publish pending tests data. On May 15, these states — Punjab, Haryana, Bihar, Chhattisgarh, Tamil Nadu, Kerala, Rajasthan, Uttar Pradesh — together tested around 36,000 samples on the day, and had a total backlog of 18,379 samples.Â
HuffPost India
A snapshot of pending tests across eight major Indian states. It is worth noting that states with the highest case counts do not publish data on pending tests.
It is worth noting that the test positivity rate of all the eight states is less than the national average, meaning none of the states where the detected infection rate is higher have shared their data on test pendency. The available numbers do not tell us how widespread the delays are, a concern that anecdotal new reports from many states have raised where patients say they have waited for upto 10 days to receive their test results.
“Delayed test results lead to delay in getting individuals timely treatment and could lead to complications; it also affects contact tracing and breaking the chain of transmission,†said Genevie Fernandes, a public health researcher and postdoctoral research fellow at the University of Edinburgh.Â
“The first government response should be transparent reporting on websites and other forums regarding the delay in test results and also explaining the reasons for the same,†Fernandes said. “The second response should be fixing this delay.â€Â
In this context, the record national spike of positive cases on May 17 doesn’t offer particularly helpful insights into the virus’s march across India — the “record†numbers simply indicate that the aggregated national level data across 36 states and union territories, each with varying degrees of delay and pendency, added up to the highest daily number till date. Â
Test positivity
 The limitations of the numbers is just one concern. The manner in which they are interpreted in public is also contested. Consider India’s low test positivity rate, which Union health officials use to reassure an anxious public that the coronavirus is not as widespread in India as it is elsewhere in the world and to deflect criticism that India, as a country, is not testing enough of its population.Â
At a press briefing on April 16, Dr Raman R Gangakhedkar, Head of Epidemiology and Communicable Diseases at the ICMR, referred to the low national positivity rate to justify the low rate of testing in India.
“In countries like Japan, one out of 11.7 tests turns out to be positive, which is among the highest in the world. Italy tests 6.7 persons for one positive test while the USA tests 5.3 persons and the United Kingdom 3.4,†Gangakhedkar said at the press conference.Â
“Taking their population base into consideration, it is difficult to comment about our testing rate,†Gangakhedkar said. “In India, we are conducting 24 tests out of which one comes out to be positive. Also, we have a huge population and not all people belong to vulnerable groups. Hence, can’t say our testing ratio is low.â€
But experts say that India’s test positivity rate is more reflective of the country’s testing strategy.
“Our testing criteria is limited. We are not conducting widespread testing regardless of symptoms, hence we will not know the true figure of those who have the infection in a population,†Fernandes, the public health researcher, said. “Hence, the assumption of reduced transmission owing to the low test positivity rate at the national level may not hold true.â€
A deep dive into state-wise test positivity rates shows the number fluctuates significantly. As mentioned earlier, in states like Maharashtra, the test positivity rate has risen significantly as the government expanded testing, while Tamil Nadu has witnessed the opposite trend.
Perhaps the most vivid example of the unpredictability of test positivity trends, and a good reason to test as widely as possible, is the case of Bhilwara in Rajasthan which gathered national attention as one of the first hotspots, and was subjected to what was described as a â€ruthless lockdownâ€.Â
Today, the district with 2.8 million population has done 15,993 tests—5,711 tests per million, more than three times the national average— with a test positivity rate of just 0.5%, ten times lower than the national figure.Â
“The national figure definitely makes no sense in the context of a disease which is spreading very differently in different parts of the country,†Menon of Ashoka University said, referring to the wide variation in the test positivity rates.Â
Modelling woes
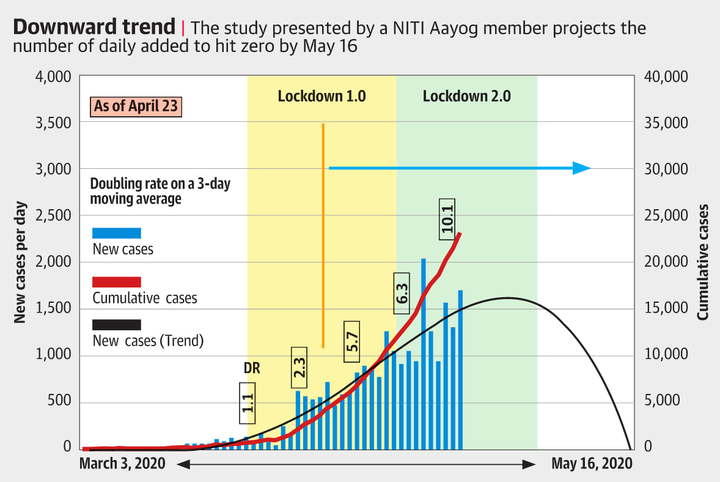
At a press conference on April 24, VK Paul, NITI Aayog and head of a government empowered committee on medical management, displayed a surprising slide suggesting the number of new cases would go to zero on May 16, which, according to The Hindu, members of Paul’s own committee didn’t agree with. May 16, coincidently, was a day before Prime Minister Modi’s second extension of the lockdown was scheduled to end.
Paul subsequently walked back his remarks in a statement to Caravan, suggesting “that was a trend line†without offering any further details, but the slide is a worrying illustration of the quality of the modelling and future projection scenarios panning out in India that are central to managing the pandemic response.Â
“Those were ridiculous predictions, especially because the methodology that led to them has never been disclosed,†Menon said. “So it is impossible to say whether there is a real epidemiological model behind them or not. Anyone can plot a function that runs through a given set of points.â€Â
HuffPost India
Experts say government projections such as this slide presented before the media on May 16 make a mockery of attempts to model the coronavirus’s spread across the country.
The government’s own internal projections, shared amongst officials but not with the press, suggest that the public claims are carefully choreographed to manage the national narrative.Â
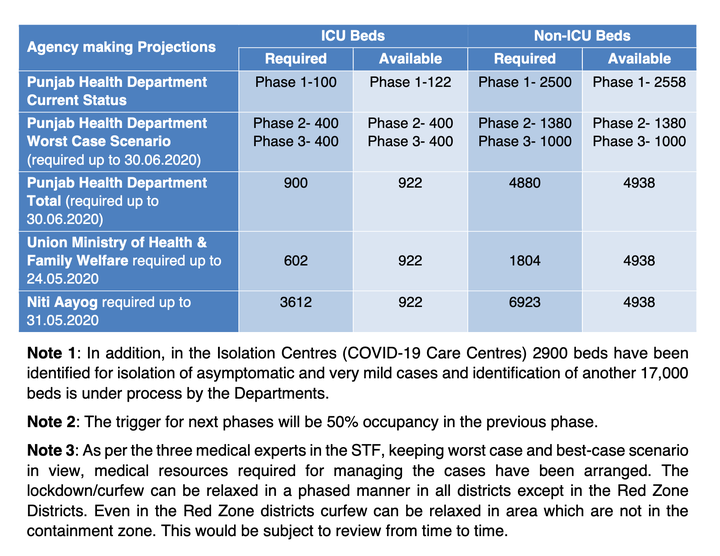
Take Punjab. According to the task force report on the existing lockdown strategy released on April 25, the state was presented with three different projections: from the Punjab’s health department, NITI Aayog and the Union health ministry.
The health ministry projections for Punjab said the state would need 602 ICU beds by 24 May while NITI’s estimate was six times, at 3612 beds. In fact, NITI— of which Paul is a member—told the state to expect 3,680 new cases per day from 31 May.Â
HuffPost India
A slide from a Punjab government presentation revealing widely diverging projections on the health infrastructure required to tackle the crisis.Source: Exit Strategy for COVID-19 Lockdown Restrictions, Punjab Task Force / 25 April 2020
An official who helped the state task force said Punjab had not been provided details on how these projections were arrived at, which meant they could not reconcile why the numbers from the Centre were significantly higher than the state’s own health department.Â
“Data science should be transparent. All models are wrinkled with assumptions but it should be clear what the assumptions are,†said Bhramar Mukherjee, a professor and chair of biostatistics at the University of Michigan.
The opacity of much of India’s modelling does not allow external experts to evaluate the built-in assumptions—a critical component of improving the models. Neither is the public informed of the basis on which decisions are being made.Â
Models, Mukherjee said, should not be quoted or taken as destiny for their exact numbers as there are huge uncertainties associated with the projections, but to help decision makers evaluate likely scenarios based on possible interventions.Â
Thus far, details of only one modelling project, MedInventory—which was facilitated by Principal Scientific Advisor to the Prime Minister—are in the public domain. It provides district-wise projections for the healthcare infrastructure requirement in the next four weeks. However, it is not clear who is using it.Â
Health officials of three states—Telangana, Andhra Pradesh and Tamil Nadu— told HuffPost India they were not using the MedInventory website. Instead, agencies at different levels of government are making their own projections.Â
“Even though the state had also requested the Ministry of Health for projections in April, Andhra Pradesh has been relying on its own projections arrived at by expert committees which have access to data compiled by the state,†a state health official of Andhra Pradesh explained. “Based on the state’s projections, AP has readied a total of 50,000 beds for Covid-19 patients for June-July.â€
Doubling rate obsession
Across the country, most health officials continue to speak in terms of “doubling ratesâ€, the time taken for the number of COVID-19 cases to double in number, to make future projections.Â
“We are keeping track of the doubling rate,†said Pradip Awate, state surveillance officer of Maharashtra. “ As of May 13, it stands at 10.2 days. So if we have 24,000 cases today, we are projecting 48,000 cases after 10 days, and accordingly we think of the capacity needed.â€Â
Awate said the state does not make district-wise projections.Â
But experts raise questions about this metric.Â
“The doubling time is a crude measure. It is a measure on the relative scale,†Mukherjee from the University of Michigan said.Â
“For prioritization and resource allocation you need an idea about total case-counts, hospitalization counts and estimated counts for those that will seek critical care. I am not sure how ‘doubling time’ will help with these projections,†she said.Â
“I wish there were more savvy statisticians working closely with the government,†Mukherjee said.Â
Menon, the Ashoka University professor, said that the doubling rate is not a bad proxy in the early part of the epidemic when the disease is in its exponential growth phase to tell what might happen in the next few days. “But once the case numbers begin to drop, this approach will of course make no sense at all,†he explained.Â
“The doubling rate ignores the fact that the disease spreads at different rates in different places,†Menon said. “It will spread slowly in places where physical distancing is taken seriously, mask wearing is common and hand-washing and similar measures are prevalent. It will spread fast in dense crowded regions where none of these is attended to.â€Â
“So to use a single doubling rate across a whole state can mask the growing number of cases in districts and sub-districts, since it is a less granular measure,†Menon said.
Over a long period of 6 to 8 months, Awate, the Maharashtra official said, the state is expecting 0.5% of its residents to be infected with the virus, of which 15% would need hospital treatment and 5% would need critical care—and the state is ramping up its healthcare capacity accordingly.Â
“We are hoping for the best and preparing for the worst,†Awate said.Â
— With inputs from Nikhila Henry in Telangana
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
“They noted overnight ‘online traffic and conversion have exploded in the past six weeks with a 63 per cent jump in new online customers’,†said Mr Mitchell.
RBC analysts said Afterpay’s latest trading update suggested 2020 financial year consensus forecasts “have been cut too far in recent months,” but the share price showed markets have “arguably shrugged this off, reflected in valuation multiples sitting back at the top end of historical ranges.”
Record highs
Afterpay’s stock has been testing record highs since WeChat owner Tencent emerged with a 5 per cent stake this month, which was interpreted both as a validation of the deferred payment concept and an opportunity to use the investor as a potential partner to expand into new markets.
Afterpay’s stock traded 4.3 per cent higher at $44.72 at about 10:30am on Thursday in Sydney.
Analysts had already flagged Afterpay’s stellar progress in the US. Citi reported this month that Afterpay’s web site visits increased 208 per cent in April – compared to April 2019 – and noted “Afterpay also overtook [Commonwealth-Bank-backed rival] Klarna to have the highest app downloads in the US.”
“At a time in which ecommerce has become the primary way people are shopping, there is a growing interest and demand among consumers to pay for things they want and need over time using their own money – instead of turning to expensive loans with interest, fees or revolving debt,” said Afterpay co-founder Nick Molnar.
Growing confidence
The company said that on average, its merchant partners saw customer conversion rates on sales [customers paying to complete their purchases] lift by more than 20 per cent, and average order values increase more than 25 per cent compared to all other payment methods.
The Tencent investment hasn’t been the only factor driving Afterpay’s shares to record highs.
Investors are growing increasingly confident that the COVID-19-induced recession will not be a near-death experience for the buy now pay later sector as customers lose their jobs and their ability to buy and pay for goods using the service.
Loading
Rival Zip reported that its business actually received a boost as customers and merchants were forced to transact online.
“The key question is whether the momentum and shift to e-commerce persist,” said Citi’s Siraj Ahmed. “If the current trends continue, then we see upside risks to our [second half FY2020 forecasts] for GMV [gross merchant volume] forecast of $5 billion … and active customer forecast of 9.3 million.”
RBC, with a 12-month share price target of $29 for Afterpay, is more cautious.
“We feel plenty of growth is factored in at these levels, however we acknowledge the current structural tailwinds and probably won’t get a good feel for loss rates until the large government stimulus programs roll off later in the year,” its analysts said.
Ophir’s Mitchell also expressed some caution and said his firm will be closely watching how these trends play out longer term.
“We are keeping a keen eye on whether online will slow as bricks and mortar [shops] reopen, and what this will do to overall customer growth,†he said.
Colin Kruger is a business reporter. He joined the Sydney Morning Herald in 1999 as its technology editor. Other roles have included the Herald’s deputy business editor and online business editor.
Fox News host Dana Perino got more than she bargained for on Wednesday when she challenged Biden campaign adviser Symone Sanders to provide “one example of a lie from the White House on the coronavirus pandemic.â€Â
Perino had played comments from presumptive Democratic presidential nominee Joe Biden’s virtual commencement address for Columbia Law School on Wednesday, during which Biden said, “You can build a truly representative democracy with more facts than lies.â€
“So, I’m assuming that former Vice President Biden is saying that President Trump is the one that he’s talking about there, and lies about the coronavirus,†Perino said. “What specifically would he be talking about?â€
Sanders responded that there has been a lot of misinformation about the virus, and “some of it, in fact, has come from the White House.†She pointed out the Trump administration’s failure to “act quickly and with urgency†in January and February. Biden would continue to call these failures out, Sanders added.
“But you, you don’t have [a lie] off the top of your head? I can’t think of one,†Perino insisted. “I would just like even one example of a lie from the White House about the coronavirus pandemic,†she added after Sanders noted there were “so many†to choose from.
Pretty great: Dana Perino thinks she’s gonna stump @SymoneDSanders into a viral moment of being unable to name check a Trump lie on coronavirus. Instead, Symone rattles off so many that Perino has to interject to change the subject.pic.twitter.com/FxN1q2Uf8K
Sanders quickly listed two things Trump had lied about: testing availability and access to personal protective equipment.
“Everyone that wants a test can get a test. How about that lie? Because everyone who wants or needs a test in this country is not able to access testing,†she said.
“How about all the governors have the PPE and the ventilators that they need? We know that’s not true. There are folks in places from California to Michigan to Florida and in between who are sewing masks for front-line workers because they don’t have the proper PPE.â€
Perino conceded that the lack of PPE was an issue. Sanders noted that those were just a couple of lies from the president, adding, “I don’t want to take the whole interview to run through them.â€
“No, I don’t either,†Perino concluded.
Watch the exchange above.
A HuffPost Guide To Coronavirus
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
Ismael Fernández thought his pet donkey Baldomera would not remember him after he had been under quarantine, but the beloved animal gave him an unexpectedly emotional reunion.
Michael Cohen, President Donald Trump’s former fixer and longtime attorney, will be released from prison early and serve the remainder of his three-year term under home confinement, according to multiple media reports.
Cohen will be released from a facility in New York later this week, The Wall Street Journal reported. He has served about a year of his sentence after being convicted on charges of lying to Congress and violating campaign finance laws when he directed hush-money payments to women who said they had sex with Trump. Cohen was scheduled to be released in November 2021.
Cohen’s attorneys initially asked the courts to let him serve the remainder of his sentence at home as the coronavirus began to spread, but a federal judge rejected the request, saying he believed the plea was “just another effort to inject himself into the news cycle.â€
The Associated Press reported last month, however, that Cohen was scheduled to be released early as the outbreak grew. The Bureau of Prisons has the authority to release inmates to home confinement without a judicial order.Â
As the coronavirus spread around the nation, Attorney General William Barr ordered the Bureau of Prisons last month to expand its guidelines for prisoners who are eligible for early release or home confinement. Barr said the agency should work to protect “the most vulnerable†in affected facilities.
“We are experiencing significant levels of infection at several of our facilities,†Barr wrote in a memo obtained by Politico. “We have to move with dispatch in using home confinement, where appropriate, to move vulnerable inmates out of these institutions.â€
More than 1.5 million people in the U.S. have tested positive for COVID-19. Prisons and jails have been hit hard by the virus due to their low rates of testing and inconsistent reporting of outbreaks, according to investigations.
Several other high-profile people have been released from prison in recent weeks, including Paul Manafort, Trump’s former campaign chairman, and Michael Avenatti, who represented Stormy Daniels, one of the women who received a hush-money payment from Cohen.
The Bureau of Prisons has more than 137,000 federal inmates and 36,000 staff members. The agency says more than 2,200 inmates had tested positive for COVID-19.
A HuffPost Guide To Coronavirus
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
Whether it’s advisable or not, many people going stir crazy from weeks of social distancing are looking to take a drive or even a road trip.
Though the Centers for Disease Control and Prevention recommends that people restrict car travel to essential trips only, folks are ready to skirt the rules a little. About 1 in 3 Americans are planning to take a road trip this summer, according to a recent survey conducted by travel app GasBuddy. (The lower gas prices of the last few months have made road travel extra alluring, but don’t get too used to it. As states reopen, gas prices are slowly creeping back up.)
If you are jonesing to travel, there are precautions you should take to make your trip a little safer. Below, health and travel experts offer their best advice on how to hit the road in the age of COVID-19.
Consider taking a shorter trip. If it’s longer, plan the trip to a T.
Gauge the risk factors involved in traveling away from home for however long you’re out: Do you have a weak bladder that’s going to require lots of bathroom breaks? Are you in a high-risk group for the coronavirus? How many people are in the car? What is their health status? (The bottom line remains that the more people who go, the more opportunities for others to contract the virus.) How long will you be out there?
“Longer distances may mean more stops and more exposures, but if you take precautions you can minimize your risk of exposure,†said Rachel Patzer, an associate professor at Emory University School of Medicine.
Jose A. Bernat Bacete via Getty Images
Plan your trip as thoroughly as possible.Â
Prepare for those dreaded bathroom breaks.
Let’s address the elephant in the room: If you can’t hold it, what are some best practices for using a public toilet? Gas stations, which are essential businesses, may be your only option for restroom facilities. While hopefully they’re cleaned often and well stocked with toilet paper, prepare for the worst by bringing your own TP and soap.
In fact, it’s not a bad idea to bring a whole emergency kit that includes hand sanitizer, toilet paper, soap and travel-size packs of toilet seat covers, said Krutika Kuppalli, an infectious diseases physician and biosecurity fellow at the Johns Hopkins Center for Health Security.
No judgment if you want to hover over the toilet in a squat. After using the bathroom, wash your hands like you’ve been chopping jalapeños all day and really need to get it all off you.
“Use extremely good hand hygiene if you go to the restroom,†Kuppalli said. “Remember, we know that you get infected with the virus via infection of the mucous membranes ― eyes, nose, mouth.â€
Per the CDC guidelines, wash for 20 seconds, use a clean disposable paper towel to turn off the faucet, and then wipe your hands dry.
If you have kids who have trouble not touching everything in sight, Patzer recommends bringing a potty training chair in the trunk of your car.
“We used to do this for long trips when our kids were younger anyway because they never liked to use the public toilets!†she said.
RealPeopleGroup via Getty Images
Wash your hands thoroughly when using a public restroom. Don’t forget your mask, either.Â
Do more research about your route than you normally would.
The CDC recommends checking with the state or local authorities where you are, along your route and at your planned destination to learn about any local issues or travel restrictions. Federal law cannot bar you from traveling to another state, but local authorities can require self-quarantine for as long as 14 days once you arrive. (To check whether the state you’re planning to visit has such a policy, call the state health authority on this handy list provided by the CDC.)
Identify whether rest stops are open along your route, said Jim Stratton, the public relations manager at AAA National. The closures vary from state to state.
It’s also a good idea to check the COVID-19 infection rates for the counties you’re considering driving through and to, said travel writer Wendy Perrin.
“Basically, you want to know where the hot spots are so you can avoid them,†she told HuffPost.
Pick a destination that shouldn’t be too crowded ― and have a Plan B if there are too many people there.
When determining where you’ll go, outdoor places with wide-open spaces and a lot of fresh air are obviously ideal. In many states, hiking trails and other outdoor recreational areas are now open. Just consider whether your destination might be swarmed with people.
“If you know a park or beach is popular, stay away from them right from the get-go,†Perrin advised. “Instead, choose lesser-known nature destinations so that social distancing is easier.â€
But you might still arrive at your go-to spot and find it full or closed. It pays to have some backup plans in mind, especially if you have a car full of antsy kiddos.
Aim for less-populated recreational sites right now.Â
When you get gas, be aware of high-touch areas.
If you’re pumping gas, gloves are a smart idea ― the gas pumps could be contaminated from frequent use. Dispose of those gloves in a nearby trash container, not on the ground. (We never thought we’d have to say that, but people are throwing them everywhere.)
Kuppalli said she’d also be concerned about high-touch areas where the virus could live in your own car: the steering wheel, the cup holders, the buttons you press to change the radio station or control the air conditioning, the dashboard and the seats. They’re all worth cleaning with sanitizing wipes or a soapy paper towel.
Make sure your car is up to the stress of a long drive.
Before any lengthy road trip, AAA advises drivers to have a full vehicle inspection, making sure fluids are topped off and there isn’t any underlying issue that could cause a breakdown. Stratton has a simple acronym to remind drivers off what needs to be checked before heading out.
“All drivers should make a good B-E-T to keep their road trips on track by having a car’s battery, engine and tires checked before embarking on a long trip,†he said.
A battery on the brink of dying rarely warns a driver before it fails, but a simple battery test can uncover potential problems, Stratton said. (AAA offers its members free testing of a vehicle’s battery.)
Additionally, have a well-stocked emergency kit on hand. Stratton recommends including a cellphone car charger, a flashlight with extra batteries, a first-aid kit, a jug of drinking water, extra food for people (and pets, if you’re bringing them), jumper cables, and emergency flares or reflectors.
Guido Mieth via Getty Images
It’s not a bad idea to check your car’s oil status before heading out.
If it’s a long trip, prepare to use rest stops or possibly stay at a hotel.
If your trip is more than just a quick jaunt to the beach or the mountains for a hike, you’ll want to take the occasional break. If it’s especially long, you may need to stop somewhere for sleep, so you’re not driving drowsy. (According to the National Safety Council, more than 100,000 accidents in 2019 were the result of drowsy driving.)
To that end, call ahead to make sure that rest stops you’re familiar with are open.
If you plan to stay at a hotel or motel (also call ahead), be extra cautious. Clean high-touch areas in the room, like doors, tables, faucets, toilets, sinks, light switches, phones, remotes and curtain handles, Kuppalli said.
“Just like with public bathrooms, I recommend bringing sanitizer wipes to wipe down all of these high-touch areas in case the hotel hasn’t done that,†she said.
If you don’t have a car but really need to get away, some options are better than others.
Your safest bet if you don’t own a car is to rent a vehicle.
Perrin recommends turning on the air conditioning and rolling down the windows so you’re not breathing in the last driver’s air. And of course, wipe down all those high-touch areas mentioned above.
If you’re not renting a car, consider Uber or Lyft, Kuppalli suggested.
“Just make sure you’re wearing a mask,†she said. “You could also consider a train depending on what type of options are available. For instance, sleeper cars may have better options for physical distancing.â€
However you travel, plan on being as self-sufficient as possible on the road.
“Bring everything you might need with you to minimize stops and reduce services en route,†Perrin said. “Water, snacks, lunch, disinfectant wipes, mask, extra mask, gloves, extra gloves, phone charger, Ziploc bags, a towel or even a change of clothing.â€
“Take whatever you might need,†she said. “You really want to factor in a range of ‘what if’ scenarios.â€
Experts are still learning about the novel coronavirus. The information in this story is what was known or available as of press time, but it’s possible guidance around COVID-19 could change as scientists discover more about the virus. Please check the Centers for Disease Control and Prevention for the most updated recommendations.
Ruby Rose is leaving her groundbreaking role on “Batwoman†after just one season.
Rose, who portrayed the first queer title-role superhero on a live-action TV series, said in a statement:
“I have made the very difficult decision to not return to ‘Batwoman’ next season. This was not a decision I made lightly as I have the utmost respect for the cast, crew and everyone involved with the show in both Vancouver and in Los Angeles.â€
Neither Rose nor the producers indicated why she was departing. Deadline suggested the parting was mutual and was unrelated to a stunt injury in which she said she herniated two discs and underwent emergency surgery to avoid potential paralysis. Variety, citing an unnamed source, said Rose’s health was not a factor.
The grind of playing a lead had taken its toll on the “Orange is the New Black†alum, according to Deadline.
Rose, who had played Batwoman before, made history when the CW announced it was picking up a full series featuring Batwoman in May 2019. “Batwoman†became the first superhero live-action TV series to feature a gay or lesbian title character.
The coronavirus pandemic has pushed the second-season premiere of “Batwoman†to January 2021, leaving producers with sufficient time to recast the lead. They pledged in a statement to fill the role with an actor who, like Rose, is from the “LGBTQ community.â€
WASHINGTON, May 20 (Reuters) – Nancy Pelosi, the top elected U.S. Democrat, compared President Donald Trump on Wednesday to a child “with doggy doo on his shoes,†as the spat between the two leaders escalated.
The speaker of the U.S. House of Representatives and the Republican president have not spoken directly for seven months but have exchanged barbs this week as Congress and the White House work to respond to a coronavirus pandemic that has killed more than 91,000 people in the United States.
“It’s like a child who comes in with mud on their pants,†Pelosi told a news conference when asked about provocative comments Trump has made about MSNBC television host Joe Scarborough, including references to him as “psycho.â€
“He comes in with doggy doo on his shoes and everybody who works with him has that on their shoes, too, for a very longtime to come,†Pelosi said, referring to canine excrement.
Trump, famous for his name-calling and insults, toldreporters earlier in the week during a visit to Capitol Hill: “Pelosi is a sick woman. She’s got a lot of problems. A lot of mental problems.â€
The president was responding to Pelosi’s comments on Monday that he should not be taking the malaria drug hydroxychloroquine as a preventive medicine against the coronavirus because of his age and being in a weight group she said was “morbidly obese.â€
Pelosi, who is second in line for the presidency, has not spoken directly to Trump since Oct. 16, when she attended aWhite House meeting on Syria.
Treasury Secretary Steven Mnuchin and other Trump administration officials led the negotiations with Pelosi and other congressional Democrats that resulted in $3 trillion in coronavirus relief over the past two months.
(Reporting by Richard Cowan; Editing by Scott Malone and Peter Cooney)
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
A major clean-up operation is continuing in Geelong after a powerful storm cell ripped rooves off homes, uprooted trees and littered debris following another night of heavy rain.
Severe weather experts have travelled to the Victorian city to investigate what caused this storm, which was possibly a mini tornado.
Meteorologists say wind gusts reached 150kms/h causing damage to at least 100 homes.
Geelong suffered another night of severe weather that left about 100 homes damaged. (Nine)Residents in Geelong face big damage bills after a storm ripped through the city. (Nine)
The hardest-hit areas were Waurn Ponds and Mt Duneed near Geelong.
Residents of damaged homes faced a race against time to protect their properties from heavy rain that fell overnight and is forecast to continue today.
It followed Tuesday night’s severe weather in the area that damaged an estimated 60 properties.
Volunteers spent Wear Orange Wednesday, the day of thanks to the State Emergency Service, assessing the damage.
Weather experts are investigating the cause of the severe weather in Geelong. (Nine)CCTV captures lightening in Geelong. (Supplied Nine)
The Bureau of Meteorology said a strong cold front moved across the state on Tuesday night, bringing the line of thunderstorms and lightning.
Victorians should expect more rain over the coming days, but no severe storms would arrive with it and further damage was unlikely.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.