{kind=link}
Introduction
The COVID-19 epidemic brought on by SARS-CoV-2 has turn into a worldwide problem for the worldwide well being system.1 Present downside associated to COVID-19 is varied issues after COVID-19, particularly long-term mortality after COVID-19. In accordance with research, mortality through the subsequent yr is comparatively greater in individuals who have had COVID-19 in comparison with those that remained uninfected, particularly elder individuals and other people with persistent ailments.2,3
Earlier research have targeted on the seek for common markers of mortality prognosis within the early interval of COVID-19. Authors demonstrated that the comorbidity and severity of COVID-19 contribute extra to mortality,4 both an impartial predictor of cardiovascular issues5,6 kidney issues7 or different issues.8
Nevertheless, these days the stratification of COVID-19 sufferers within the early levels and the forthcoming interval stays not totally understood, and the seek for essentially the most correct biomarkers to foretell the mortality of sufferers with COVID-19 continues. It was demonstrated the significance of routine blood check, that are efficient within the analysis, prognosis and mortality of COVID-19.9,10
In accordance with current research, the Neutrophil-to-Lymphocyte ratio (NLR) has predictive worth in diagnosing and predicting severity and mortality in sufferers within the early interval of COVID-19, which can assist in threat stratification fashions to foretell extreme and deadly outcomes.11,12 Typically, the NLR check is a quantitative ratio between the innate and adaptive immune programs that expresses the fundamental stability of the immune system which affiliate with the end result of infectious or inflammatory ailments and issues.13,14
Set off receptor expressed on myeloid cells-1 (TREM-1) is an immune receptor expressed by neutrophils, macrophages, and mature monocytes that may be activated in inflammatory ailments as an enhancer of pro-inflammatory innate immune responses in response to bacterial flora and have been first described as a promising marker of sepsis.15 Soluble TREM-1, sometimes called sTREM-1, represents its cleaved and circulating soluble counterpart. sTREM-1 is a preferential biomarker of febrile mortality in comparison with classical inflammatory markers.16,17 Additionally, there are a number of makes an attempt to research TREM-1 in non-communicable ailments.18,19 Furthermore, sTREM-1 is now identified to be a predictor of severity and mortality within the acute section of COVID-19.20–22 Nevertheless, TREM-1 alone as a biomarker isn’t sufficient to foretell mortality within the acute interval of COVID-19.
These days, all research have targeted on the predictive worth of those markers on short-term mortality in sufferers with COVID-19. Nevertheless, there are nonetheless no research that look at these markers to foretell long-term mortality after COVID-19. It’s hypothesized that immune-mediated markers equivalent to TREM-1 and NLR can predict early and long-term mortality after COVID-19. Our examine goals to research the affiliation of immune-mediated markers TREM-1 and NLR as stratification predictors that may predict early and forthcoming mortality throughout COVID-19.
Supplies and Strategies
Research Setting and Participant Enrollment
A potential examine was carried out to enroll sufferers with COVID-19 who have been hospitalized between Might and August 2021 within the infectious ailments clinic of Karaganda regional scientific hospital and Karaganda Medical College Hospital (Kazakhstan). Inclusion Standards: (1) Adults over 18 years of age, (2) PCR-positive for COVID-19 nasopharyngeal swab. We excluded pregnant or lactating ladies, immunocompromised sufferers (human immunodeficiency virus an infection, energetic remedy for malignancies). A complete of 283 sufferers have been included within the closing evaluation (Determine S1).
We collected all sufferers’ knowledge from digital medical information on the course of the illness, comorbidity, anthropometric parameters, blood stress (BP), coronary heart fee (HR), oxygen saturation, laboratory exams, lung harm, intensive care unit (ICU) keep, and mechanical air flow assist. The examine solely concerned sufferers with lung tissue harm. To raised decide the severity of COVID-pneumonia in predicting mortality, we utilized chest pc tomography (CT) knowledge (% harm). This technique is straightforward to entry and supplies a easy technique to assess harm to lung tissue. CT knowledge have been visually categorized by radiological severity in response to the diploma of pulmonary involvement utilizing the RAD-Covid rating.23 All sufferers have been calculated with physique mass index, and Charlson comorbidity index.24 All investigations have been carried out on the primary day of hospitalization. Discharged sufferers have been monitored by telephone and by gathering info within the medical info system, the place all instances of remedy and/or dying of sufferers are recorded. Because the endpoint was taken all deaths from all non-specific and particular causes, taking into consideration the etiology and date of dying. The follow-up interval was 180 days from hospital admission: 30 days post-hospital to evaluate early mortality and extra 5 months follow-up of surviving sufferers to report late mortality. Sufferers who have been nonetheless alive 180 days after the hospitalization have been outlined as surviving.
The examine was permitted by the Bioethics Committee of Karaganda Medical College No. 18, dated 14 April 2021. Written knowledgeable consent was obtained from the individuals.
Immunological Evaluation
Blood samples have been collected in tubes with EDTA on the primary day after admission to the hospital. Serum aliquots have been saved in a freezer at −80°C till evaluation. sTREM-1 stage was measured utilizing a human sTREM-1 ELISA Equipment (Abcam) following the producer’s directions. The blood check was carried out on a Mindray hematological analyzer. The neutrophil–to-lymphocyte ratio (NLR) was calculated as absolutely the variety of neutrophils divided by absolutely the variety of lymphocytes.
Statistical Evaluation
Statistical evaluation was carried out utilizing Statistical Package deal for the Social Sciences (SPSS) 21.0 (IBM SPSS Statistics). Knowledge introduced in tables and graphs have been carried out utilizing Prism Model 7 software program (Graph-Pad, La Jolla CA). Regular distribution was carried out utilizing the Kolmogorov–Smirnov check. Quantitative indicators, given the non-normal distribution, are described utilizing the median (Me) and the interquartile vary. Qualitative options are described utilizing percentages. Variations between the teams have been evaluated by Kruskal–Wallis, Mann–Whitney U-tests with Bonferroni correction for a number of comparisons, or chi-square check, as applicable. Components related to the event of mortality inside 30 and 180 days have been analyzed utilizing univariate and multivariate regression. Predictor accuracy was decided by the realm below the curve (AUC) of the receiver working attribute (ROC). AUCs with 95% confidence intervals have been calculated to estimate the diagnostic worth of NLR and sTREM-1. The classification threshold or the cut-off worth was decided utilizing ROC evaluation, similar to the purpose on the ROC curve with the best sensitivity index and the bottom worth of false optimistic outcomes. The desired level on the curve was decided utilizing the calculation of the Youden’s index. Hazard ratios have been based mostly on Log rank exams (Cox regression). The p-values are given within the tables, and p < 0.05 is taken into account statistically vital.
Outcomes
Demographics, Scientific and Laboratory Traits of Sufferers
There have been analyzed Knowledge from 283 sufferers with COVID-19 in an infectious ailments hospital. The scientific traits of sufferers are introduced in Desk 1. 23 individuals died: over a 30-day interval – 13 individuals (4.6%), the median was 12 days; for an additional 6 months – 10 individuals (3.5%), the median of 56 days. The imply age of deceased sufferers at 30 and 180 days was greater than that of surviving sufferers (p=0.0001). There have been no gender variations between the deceased and the survivors. The Charlson comorbidity index didn’t differ between survivors and deceased over a 30-day interval, whereas sufferers who died inside 6 months of sickness had a better comorbidity index than survivors (p=0.002). The proportion of lung harm in response to CT was greater within the group of the deceased (p=0.007): in sufferers with 30-day mortality – 45 (28–60), within the deceased group inside 180 days – 38 (17–50), among the many survivor’s group lung harm was 25 (10–37). Oxygen saturation ranges in 30- and 180-days deceased sufferers have been decrease (p=0.047), and respiratory fee (p=0.0001) have been additionally greater than within the survivor’s group. Furthermore, sufferers with a deadly consequence have been extra typically transferred to the ICU (69.2% and 40%) and obtained respiratory assist (69.2% and 30%). The imply size of hospital stays for sufferers with COVID-19 didn’t differ between teams.
|
Desk 1 Scientific and Demographic Knowledge of Sufferers with COVID-19 Included within the Research |
The variations in laboratory markers between teams have been detected: neutrophils depend, D-dimer ranges, and acute section proteins (ferritin, CRP) have been greater within the group of sufferers with early and late deadly outcomes (Desk 1).
The etiology of early mortality was: cardiopulmonary insufficiency (77%) and cerebral edema (23%); within the etiology of late mortality: cardiopulmonary insufficiency additionally prevailed (80%), cerebral edema was much less widespread (10%), dying from different causes was 10%.
Prognostic Utility of sTREM-1 and Neutrophil-to-Lymphocyte Ratio on Mortality
Greater plasma concentrations of sTREM-1 in deceased sufferers at 30 days in contrast with survivors have been 87.41 (63.9–117.12) pg/mL versus 59.18 (41.83–84.48) pg/mL, p=0.003 (Determine 1A). Equally, deceased sufferers at 6 months had greater sTREM-1 plasma concentrations in comparison with survivors of 93.11 (52.26–140.27) pg/mL versus 59.18 (41.83–84.48) pg/mL, p=0.0001.
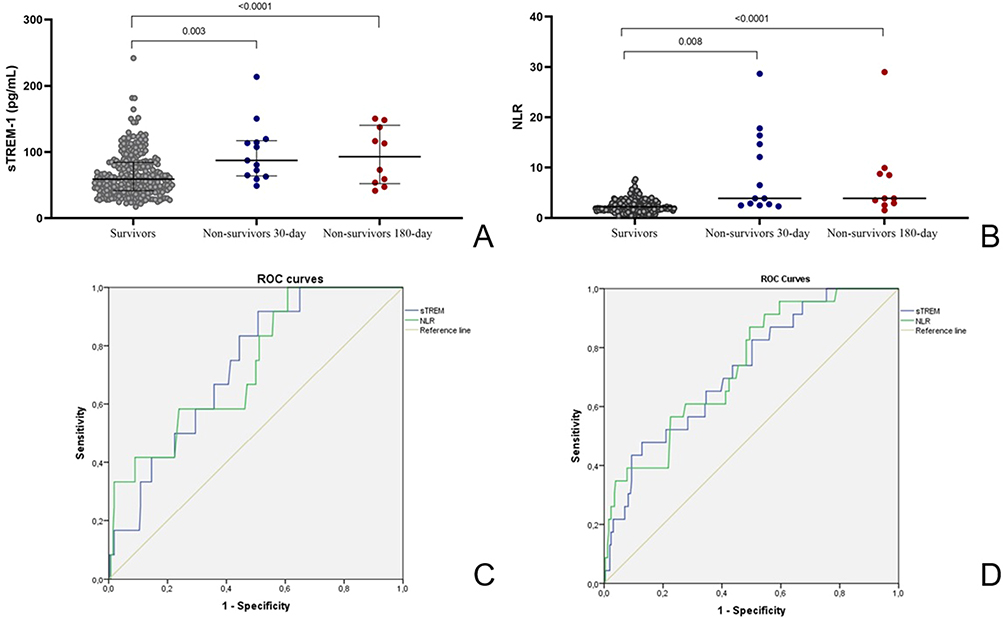 |
Determine 1 The plasma focus of sTREM (A) and NLR (B) in COVID-19 survivor sufferers, non-survivors 30-day, and survivors 180-day was analyzed and in contrast. Knowledge are introduced as imply values plus ranges. Mann–Whitney U-test was used to carry out comparisons with Bonferroni correction for a number of comparisons. Variations between the teams are indicated by the p-value; (C) ROC curves for sTREM (blue) and NLR (inexperienced) for predicting the short-term mortality of COVID-19; (D) ROC curves for sTREM (blue) and NLR (inexperienced) for predicting the long-term mortality of COVID-19. |
Compared with NLR between teams of survivors and deceased, the next statistical variations have been discovered (Determine 1B): NLR within the group of those that died inside a month – 3.89 (2.50–15.53), inside 6 months – 3.89 (2.81–9.06), which is considerably greater than within the group of survivors – 2.46 (1.62–3.73).
The predictive worth of sTREM-1 and NLR in sufferers with COVID-19 was assessed by ROC curves. The ROC curve for survivors and deceased teams over a 30-day based mostly on sTREM-1 concentrations and NLR ranges is introduced in Determine 1C. The traits of the ROC assay are introduced in Desk 2. The cut-off for sTREM-1 was calculated at 59.08 pg/mL with 92% sensitivity and 49% specificity, and the cut-off for NLR was 2.29 (92% sensitivity and 49% specificity). AUC for sTREM-1 was 0.744 (95% CI: 0.632–0.856), and for NLR 0.717 (0.589–0.844), indicating reasonable discrimination between survivors and deceased teams.
 |
Desk 2 Significance of sTREM-1 and NLR at Admission in Predicting Quick- and Lengthy-Time period Mortality in Sufferers with COVID-19 |
The ROC curve of sTREM-1 and NLR ranges for survivors and deceased teams over a 180-day is proven in Determine 1D. The cut-off of NLR was >2.10 and TREM-1 >47.34 have AUC values of 0.737 (95% CI 0.637–0.836) and 0.726 (95% CI 0.623–0.828), respectively (Desk 2).
Regression evaluation to foretell mortality and significance of sTREM-1 and NLR at admission in predicting short-term and long-term mortality in sufferers with COVID-19.
The multivariate Cox regression evaluating the connection of markers with early mortality is proven in Desk 3. After adjusting for age, comorbidity index, and proportion of lung harm, NLR and sTREM-1 scores retained a statistically vital impact on the chance of affected person mortality over a 30-day interval.
 |
Desk 3 The Univariate and Multivariate Cox Regression Evaluation to Assess Danger Components for Early Loss of life in Sufferers with COVID-19 |
Stratified evaluation of long-term mortality demonstrated that sTREM-1 (HR 1.011 (CI 1.002–1.023); p=0.049) and NLR (HR 1.062 (CI 1.004–1.124); p=0.035) retained predictive energy after mannequin adjustment for age, variety of comorbidities, and evaluation of lung harm (Desk 4).
 |
Desk 4 The Univariate and Multivariate Cox Regression Evaluation to Assess Danger Components for Lengthy-Time period Loss of life in Sufferers with COVID-19 |
Evaluation of early affected person survival, stratified for the affiliation of sTREM-1 and NLR, signifies that sufferers with a plasma sTREM-1 focus better than 59.08 pg/mL and an NLR better than 2.29 had an elevated threat of early mortality (hazard ratio = 8.07; 95% CI: 1.03–62.17 and 9.24; 95% CI: 1.202–71.08, respectively); for long-term lethality of sTREM-1 better than 47.34 pg/mL (hazard ratio = 7.96; 95% CI: 1.072–59.18) and NLR better than 2.10 (hazard ratio = 11.52; 95% CI: 1.551–85.52).
Dialogue
Knowledge from a number of impartial epidemiological research have proven that individuals who undergo with COVID-19 have a 3 times better threat of dying throughout the subsequent 6 months after the illness.25 Nevertheless, the mechanisms underlying the event of elevated mortality after COVID-19 are usually not totally understood. One of many predicted mechanisms is the affect of irritation within the acute interval of COVID-19 on mortality after the affected person’s restoration.
A hyperinflammatory response involving cytokines underlies acute COVID-19 an infection.26 Rising proof means that subsequent persistent low-grade persistent irritation could result in a persistent catabolic state and contribute to the event of long-term COVID-19.27 Elevated D-dimer, CRP, and ferritin ranges have been extra widespread in deceased and in sufferers with long-COVID than in totally recovered sufferers,28 which was additionally confirmed on this examine. It was demonstrated that vital inflammatory responses persist in sufferers even 40 to 60 days after an acute COVID-19 an infection.29 A. Mainous et al confirmed that an elevated CRP stage, which is without doubt one of the indicators of extreme COVID-19 within the acute interval, is related to an elevated threat of mortality at 12 months of follow-up.30 In accordance Morrow et al post-COVID syndrome is related to activation of the hemostasis pathway and systemic irritation throughout restoration stage.31 Then again, some research have proven no correlation between pro-inflammatory biomarkers and long-COVID syndrome.32–34
NLR and TREM-1 are complementary markers, reflecting quantitative and practical exercise of the myeloid element of innate immunity. NLR, which seems to be extra delicate than absolute neutrophil or lymphocyte depend alone in each bacterial and viral pneumonia, is a identified marker of the systemic inflammatory response for the reason that COVID-19 pandemic, the predictive worth of NLR within the improvement of extreme antagonistic outcomes in sufferers hospitalized with COVID-19 pneumonia.11–13 Moreover, sTREM-1 stage in sufferers with COVID-19 correlates with extreme illness, threat of intubation, and in-hospital mortality.20,22,35 Considerably elevated plasma ranges of sTREM-1 in sufferers with COVID-19 can point out an extreme inflammatory response and should contribute to extreme sickness and even dying.
This examine examined the affiliation of NLR and sTREM-1 with the event of deadly instances after 6 months of follow-up after COVID-19 pneumonia. It was demonstrated that the affiliation of NLR and sTREM-1 ranges with an elevated threat of dying, confirmed within the acute interval, persists regardless of the lower within the threshold values of those indicators: within the acute interval, the chance of mortality elevated with a TREM cut-off of greater than 59.08 pg/mL and NLR above 2.29, in the long run optimum cut-off TREM-1 was greater than 47.34 pg/mL and NLR above 2.10.
sTREM-1 is a receptor expressed each on the floor of blood neutrophils and on mature monocytes/macrophages that enhances the pro-inflammatory innate immune response in synergy with Toll-like receptors that acknowledge a variety of bacterial, fungal, and viral parts.36 TREM-1 activation induces elevated secretion of TNF-α, IL-6, IL-1, and IL-2 by monocytes, macrophages, and dendritic cells, which will increase irritation in infections brought on by varied pathogens.37–40 Furthermore, it has been established that sTREM-1 ranges in sepsis could mirror vital immune dysfunction, during which extreme TREM-1 cleavage could contribute to immunosuppression and dying in extreme an infection.41 Together with the established function of the sTREM-1 stage throughout acute an infection, it has been proven that the rise in sTREM-1 is the topic of intensive analysis in varied circumstances, particularly irritation.42 Accordingly, sTREM-1 ranges have been considerably related to the dangers of all-cause mortality and main cardiovascular occasions at 2 years of follow-up in post-heart assault sufferers. The exercise of matrix metalloproteinases, that are produced by myeloid cells, particularly neutrophils, was related to the chance of rupture and reworking of the center.43 Neutrophils are thought of an essential supply of sTREM-1 in infectious processes.44 sTREM-1 ranges considerably correlated with the expression of matrix metalloproteinase (MMP)-8 through the acute section of COVID-19, which might launch TREM-1 from the floor of peripheral blood cells.39 Nevertheless, the function and mechanisms of TREM-1 involvement within the improvement of post-COVID mortality want additional examine.
Older age and comorbidity have been repeatedly reported to adversely have an effect on COVID-19 outcomes.45 This examine additionally factors to an impartial impact of age on COVID-19 mortality. The imply age of deceased sufferers inside 30 and 180 days was greater than that of surviving sufferers: it was 74 years within the group of sufferers who died within the acute interval (p=0.002) and 76 years within the group with long-term mortality (p=0.0001). The affiliation impact of excessive sTREM-1 ranges with threat of long-term mortality was current for each unadjusted (HR = 1.017; 95% CI 1.009–1.025) and adjusted analyzes for age, comorbidity index, and proportion of lung tissue involvement (HR = 1.011; 95% CI 1.002–1.023).
There are some limitations in our examine. Firstly, our examine is predicated on a examine of sufferers from two hospitals positioned in the identical area. In all areas of Kazakhstan, COVID-19 remedy was carried out in response to a single protocol for analysis and remedy, and subsequently regional options shouldn’t have a major impression on irritation indicators. Secondly, the examine was observational; no evaluation was fabricated from the impact of remedy, which was extra widespread, on the chance of creating mortality within the long-term interval.46 There have been no variations within the frequency of taking medication with anti-inflammatory results within the group of survivors and people who died within the long-term interval. The examine encountered limitations because of the absence of an evaluation relating to the affiliation between elevated mortality from varied causes and sTREM-1 ranges. The examination of causes of dying amongst 3704 sufferers revealed that those that had recovered from SARS-CoV-2 confronted elevated dangers of respiratory ailments (aHR 1.9, 95% CI 1.2–3.0), malignancies (aHR 1.5, 95% CI 1.2–1.9) over 12 months, and dying from cardiovascular ailments (aHR 2.1, 95% CI 1.8–2.3).2 In our examine cardiovascular failure and acute vascular occasions emerged as the most typical causes of dying within the post-COVID interval. The examine’s limitations included the comparatively small pattern dimension in every group, posing challenges for conducting a complete evaluation of TREM-1 ranges based mostly on the causes of mortality. To handle this, the choice was made to merge the deceased group, contemplating the multiorgan harm after SARS-CoV-2, and recording dying from any trigger inside a yr.
Conclusion
Taken collectively, this examine means that early ranges of sTREM-1 and NLR are related to the chance of 6-month mortality after experiencing COVID-19. This examine expands our understanding of long-term outcomes by offering alternatives to determine a cohort of sufferers at elevated threat of dying after restoration from COVID-19. Additional analysis is required to make clear information about long-COVID-19. The obtained knowledge counsel a possible function of inflammatory markers within the improvement of extreme issues after struggling COVID-19 and stands out as the foundation for finding out the effectiveness of anti-inflammatory remedy when it comes to decreasing the chance of creating extreme manifestations of post-COVID-19 syndrome.
Knowledge Sharing Assertion
The information that assist the outcomes of this examine can be found from the corresponding creator upon cheap request.
Ethics Approval and Knowledgeable Consent
This examine was performed in accordance with the Declaration of Helsinki and permitted by the Bioethics Committee of Karaganda Medical College No. 18, dated 14 April 2021. Written knowledgeable consent was obtained from the individuals.
Creator Contributions
All authors have made vital contributions to the reported work, together with contributions to the conception, examine design, knowledge acquisition, evaluation, interpretation, and execution or in all these features. They’ve been concerned in drafting, revising, and critically reviewing the manuscript. All authors have supplied their closing approval for the model to be printed; have reached an settlement on the journal to which the article has been submitted; and have dedicated to being accountable for all features of the work.
Funding
This analysis was funded by the Ministry of Well being of the Republic of Kazakhstan, Program No. BR11065386.
Disclosure
The authors declare no battle of curiosity.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from sufferers with pneumonia in china, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. Uusküla A, Jürgenson T, Pisarev H, et al. Lengthy-term mortality following SARS-CoV-2 an infection: a nationwide cohort examine from Estonia. Lancet Area Well being Europe. 2022;18:100394. doi:10.1016/j.lanepe.2022.100394
3. Mainous AG, Rooks BJ, Wu V, Orlando FA. COVID-19 post-acute sequelae amongst adults: 12 month mortality threat. Entrance Med. 2021;8. doi:10.3389/fmed.2021.778434
4. Vlachogiannis NI, Baker KF, Georgiopoulos G, et al. Scientific frailty, and never options of acute an infection, is related to late mortality in COVID‐19: a retrospective cohort examine. J Cachexia, Sarcopenia Muscle. 2022;13(3):1502–1513. doi:10.1002/jcsm.12966
5. Wang W, Wang CY, Wang SI, Wei JCC. Lengthy-term cardiovascular outcomes in COVID-19 survivors amongst non-vaccinated inhabitants: a retrospective cohort examine from the TriNetX US collaborative networks. EClinicalMedicine. 2022;53:101619. doi:10.1016/j.eclinm.2022.101619
6. Satterfield BA, Bhatt DL, Gersh BJ. Cardiac involvement within the long-term implications of COVID-19. Nat Rev Cardiol. 2022;19(5):332–341. doi:10.1038/s41569-021-00631-3
7. Copur S, Berkkan M, Basile C, Tuttle Okay, Kanbay M. Submit-acute COVID-19 syndrome and kidney ailments: what do we all know? J Nephrol. 2022;35(3):795–805. doi:10.1007/s40620-022-01296-y
8. Oronsky B, Larson C, Hammond TC, et al. A Overview of Persistent Submit-COVID Syndrome (PPCS). Clin Rev Allergy Immunol. 2021;64(1):66–74. doi:10.1007/s12016-021-08848-3
9. Tahir Huyut M, Huyut Z, Ilkbahar F, Mertoğlu C. What’s the impression and efficacy of routine immunological, biochemical and hematological biomarkers as predictors of COVID-19 mortality? Int Immunopharmacol. 2022;105:108542. doi:10.1016/j.intimp.2022.108542
10. Zhang J, Cao Y, Tan G, et al. Scientific, radiological, and laboratory traits and threat components for severity and mortality of 289 hospitalized COVID‐19 sufferers. Allergy. 2021;76(2):533–550. doi:10.1111/all.14496
11. Alkhatip AAAMM, Kamel MG, Hamza MK, et al. The diagnostic and prognostic function of neutrophil-to-lymphocyte ratio in COVID-19: a scientific assessment and meta-analysis. Knowledgeable Rev Mol Diagn. 2021;21(5):505–514. doi:10.1080/14737159.2021.1915773
12. Parthasarathi A, Padukudru S, Arunachal S, et al. The function of neutrophil-to-lymphocyte ratio in threat stratification and prognostication of COVID-19: a scientific assessment and meta-analysis. Vaccines. 2022;10(8):1233. doi:10.3390/vaccines10081233
13. Jiang J, Liu R, Yu X, et al. The neutrophil-lymphocyte depend ratio as a diagnostic marker for bacteraemia: a scientific assessment and meta-analysis. Am J Emerg Med. 2019;37(8):1482–1489. doi:10.1016/j.ajem.2018.10.057
14. Niu D, Huang Q, Yang F, et al. Serum biomarkers to distinguish gram-negative, gram-positive and fungal an infection in febrile sufferers. J Med Microbiol. 2021;70(7). doi:10.1099/jmm.0.001360
15. Siskind S, Brenner M, Wang P. TREM-1 modulation methods for sepsis. Entrance Immunol. 2022;13. doi:10.3389/fimmu.2022.907387
16. Richard-Greenblatt M, Boillat-Blanco N, Zhong Okay, et al. Prognostic accuracy of soluble triggering receptor expressed on myeloid cells (sTREM-1)-based algorithms in febrile adults presenting to Tanzanian outpatient clinics. Clin Infect Dis. 2019. doi:10.1093/cid/ciz419
17. Su L, Liu D, Chai W, Liu D, Lengthy Y. Position of sTREM-1 in predicting mortality of an infection: a scientific assessment and meta-analysis. BMJ Open. 2016;6(5):e010314. doi:10.1136/bmjopen-2015-010314
18. Kouassi Okay, Gunasekar P, Agrawal D, Jadhav G. TREM-1; is it a pivotal goal for cardiovascular ailments? J Cardiovasc Dev Dis. 2018;5(3):45. doi:10.3390/jcdd5030045
19. Tammaro A, Derive M, Gibot S, Leemans JC, Florquin S, Dessing MC. TREM-1 and its potential ligands in non-infectious ailments: from biology to scientific views. Pharmacol Ther. 2017;177:81–95. doi:10.1016/j.pharmthera.2017.02.043
20. de Nooijer AH, Grondman I, Lambden S, et al. Elevated sTREM-1 plasma concentrations are related to poor scientific outcomes in sufferers with COVID-19. Biosci Rep. 2021;41(7). doi:10.1042/BSR20210940
21. de Sá Resende A, Matos de Oliveira YL, Rodrigues de Moura T, Martins-Filho PR. Potential function of triggering receptor expressed on myeloid cells-1 (TREM-1) in SARS-CoV-2 an infection: first insights. EXCLI J. 2021;20:722–723. doi:10.17179/excli2021-3581
22. Van Singer M, Brahier T, Ngai M, et al. COVID-19 threat stratification algorithms based mostly on sTREM-1 and IL-6 in emergency division. J Aller Clin Immunol. 2021;147(1):99–106.e4. doi:10.1016/j.jaci.2020.10.001
23. Ribeiro TFG, Rstom RA, Barbosa PNVP, et al. Tomographic rating (RAD-Covid Rating) to evaluate the scientific severity of the novel coronavirus an infection. Braz J Infect Dis. 2021;25(4):101599. doi:10.1016/j.bjid.2021.101599
24. Radovanovic D, Seifert B, City P, et al. Validity of Charlson Comorbidity Index in sufferers hospitalised with acute coronary syndrome. Insights from the nationwide AMIS Plus registry 2002–2012. Coronary heart. 2014;100(4):288–294. doi:10.1136/heartjnl-2013-304588
25. Davis HE, McCorkell L, Vogel JM, Topol EJ. Lengthy COVID: main findings, mechanisms and proposals. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s41579-022-00846-2
26. Rabaan AA, Al-Ahmed SH, Muhammad J, et al. Position of inflammatory cytokines in COVID-19 sufferers: a assessment on molecular mechanisms, immune capabilities, immunopathology and immunomodulatory medication to counter cytokine storm. Vaccines. 2021;9(5):436. doi:10.3390/vaccines9050436
27. Maamar M, Artime A, Pariente E, et al. Submit-COVID-19 syndrome, low-grade irritation and inflammatory markers: a cross-sectional examine. Curr Med Res Opin. 2022;38(6):901–909. doi:10.1080/03007995.2022.2042991
28. Huyut MT, Huyut Z. Impact of ferritin, INR, and D-dimer immunological parameters ranges as predictors of COVID-19 mortality: a robust prediction with the choice timber. Heliyon. 2023;9(3):e14015. doi:10.1016/j.heliyon.2023.e14015
29. Doykov I, Hällqvist J, Gilmour KC, Grandjean L, Mills Okay, Heywood WE. ‘The lengthy tail of Covid-19’ – The detection of a protracted inflammatory response after a SARS-CoV-2 an infection in asymptomatic and mildly affected sufferers. F1000Res. 2020;9:1349. doi:10.12688/f1000research.27287.1
30. Mainous AG, Rooks BJ, Orlando FA. The impression of preliminary COVID-19 episode irritation amongst adults on mortality inside 12 months post-hospital discharge. Entrance Med. 2022;9. doi:10.3389/fmed.2022.891375
31. Morrow AJ, Sykes R, McIntosh A, et al. A multisystem, cardio-renal investigation of post-COVID-19 sickness. Nat Med. 2022;28(6):1303–1313. doi:10.1038/s41591-022-01837-9
32. Townsend L, Dyer AH, Jones Okay, et al. Persistent fatigue following SARS-CoV-2 an infection is widespread and impartial of severity of preliminary an infection. PLoS One. 2020;15(11):e0240784. doi:10.1371/journal.pone.0240784
33. van den Borst B, Peters JB, Brink M, et al. Complete Well being evaluation 3 months after restoration from acute coronavirus illness 2019 (COVID-19). Clin Infect Dis. 2021;73(5):e1089–e1098. doi:10.1093/cid/ciaa1750
34. Moreno-Pérez O, Merino E, Leon-Ramirez JM, et al. Submit-acute COVID-19 syndrome. Incidence and threat components: a Mediterranean cohort examine. J Infect. 2021;82(3):378–383. doi:10.1016/j.jinf.2021.01.004
35. de Oliveira YLM, de Sá Resende A, Martins-Filho PR, de Moura TR. Position of triggering receptor expressed on myeloid cells-1 (TREM-1) in COVID-19 and different viral pneumonias: a scientific assessment and meta-analysis of scientific research. Inflammopharmacology. 2022;30(3):1037–1045. doi:10.1007/s10787-022-00972-6
36. Owen AM, Luan L, Burelbach KR, et al. MyD88-dependent signaling drives toll-like receptor-induced educated immunity in macrophages. Entrance Immunol. 2022:13. doi:10.3389/fimmu.2022.1044662
37. Adukpo S, Gyan BA, Ofori MF, Dodoo D, Velavan TP, Meyer CG. Triggering receptor expressed on myeloid cells 1 (TREM-1) and cytokine gene variants in difficult and uncomplicated malaria. Tropical Medication and Worldwide Well being. 2016;21(12):1592–1601. doi:10.1111/tmi.12787
38. Hommes TJ, Dessing MC, Veer C, et al. Position of triggering receptor expressed on myeloid cells-1/3 in Klebsiella -derived pneumosepsis. Am J Respir Cell Mol Biol. 2015;53(5):647–655. doi:10.1165/rcmb.2014-0485OC
39. de Oliveira Matos A, Dos Santos Dantas PH, Figueira Marques Silva-Gross sales M, Gross sales-Campos H. The function of the triggering receptor expressed on myeloid cells-1 (TREM-1) in non-bacterial infections. Crit Rev Microbiol. 2020;46(3):237–252. doi:10.1080/1040841X.2020.1751060
40. Dantas PHDS, Matos ADO, da Silva Filho E, Silva-Gross sales M, Gross sales-Campos H. Triggering receptor expressed on myeloid cells-1 (TREM-1) as a therapeutic goal in infectious and noninfectious illness: a important assessment. Int Rev Immunol. 2020;39(4):188–202. doi:10.1080/08830185.2020.1762597
41. Hotchkiss RS, Monneret G, Payen D. Immunosuppression in sepsis: a novel understanding of the dysfunction and a brand new therapeutic method. Lancet Infect Dis. 2013;13(3):260–268. doi:10.1016/S1473-3099(13)70001-X
42. da Silva-Neto PV, de Carvalho JCS, Pimentel VE, et al. sTREM-1 predicts illness severity and mortality in COVID-19 sufferers: involvement of peripheral blood leukocytes and MMP-8 exercise. Viruses. 2021;13(12):2521. doi:10.3390/v13122521
43. Kempf T, Zarbock A, Widera C, et al. GDF-15 is an inhibitor of leukocyte integrin activation required for survival after myocardial infarction in mice. Nat Med. 2011;17(5):581–588. doi:10.1038/nm.2354
44. Klesney-Tait J, Turnbull IR, Colonna M. The TREM receptor household and sign integration. Nat Immunol. 2006;7(12):1266–1273. doi:10.1038/ni1411
45. Wan EYF, Zhang R, Mathur S, et al. Submit-acute sequelae of COVID-19 in older individuals: multi-organ issues and mortality. J Journey Med. 2023;30(5). doi:10.1093/jtm/taad082
46. Noreen S, Maqbool I, Madni A. Dexamethasone: therapeutic potential, dangers, and future projection throughout COVID-19 pandemic. Eur J Pharmacol. 2021;894:173854. doi:10.1016/j.ejphar.2021.173854